- Case report
- Open access
- Published:
Multiple metastases of androgen indifferent prostate cancer in the urinary tract: two case reports and a literature review
BMC Medical Genomics volume 15, Article number: 118 (2022)
Abstract
Background
Prostate cancer (PC) is mainly known to metastasize to bone, lung and liver, but isolated metastases of prostate cancer, including ductal carcinoma, in the urinary tract are very rare. We describe two patients with nodular masses in the urinary tract (the anterior urethra or the urinary bladder) that were found on cystoscopy during treatment of castration-resistant prostate cancer.
Case presentation
In both cases, the pathological diagnosis from transurethral tumor resection showed that they were androgen indifferent prostate cancer (AIPC), including aggressive variant prostate cancer (AVPC) in Case 1 and treatment-induced neuroendocrine differentiation prostate cancer (NEPC) in Case 2. In Case 1, Loss of genetic heterozygosity (LOH) of BRCA2 and gene amplification of KRAS was identified from the urethra polyps. In Case 2, homozygous deletion was observed in PTEN, and LOH without mutation was observed in RB1.
Conclusion
These are the first reports of two cases of urinary tract metastasis of AIPC.
Background
Prostate cancer (PC) primarily metastasizes to bone, lung, and liver. Reported cases of metastases in the anterior urethra or bladder are rare, including only 15 cases of anterior urethra metastasis. Furthermore, androgen indifferent prostate cancer (AIPC), the pathological characteristics of which have increasingly been described, [1, 2] often metastasizes to similar sites, but there are no reports of urinary tract metastasis. We report two cases involving AIPC metastasis to the urinary tract, describe the genomic sequence, and discuss the potential mechanism of metastasis to the urinary tract.
Case presentation
-
Case 1. A 79 years-old man presented with obstructive lower urinary tract symptoms at another hospital. His prostate-specific antigen (PSA) level was 15.54 ng/mL. Pathological diagnosis from transrectal needle biopsy was adenocarcinoma with a Gleason Score of 5 + 5. Staging computed tomography (CT) scan showed regional lymph node (LN) metastases. He received combined androgen blockade (CAB) therapy initially, but after a decrease in PSA, his levels eventually increased. He was diagnosed with castration-resistant prostate cancer (CRPC) and began enzalutamide but despite continuous treatment for 6 months, chemotherapy was required. However, although chemotherapy initially lowered his PSA, eventually it increased a lot subsequently. He had difficulty urinating smoothly because of disease progression-related obstruction requiring clean intermittent catheterization. Subsequently, he received abiraterone but it was ineffective. Three years after the original diagnosis, he was referred to our hospital for further treatment of CRPC. He had bloody urine and difficulty with self-catheterization for 5 months after starting. Cystoscopy showed several nodular polyps in the penile urethra (Fig. 1a and b). Magnetic resonance imaging (MRI) demonstrated that the tumor had grown to 8 cm in diameter and invaded the rectum (Fig. 1c). MRI also showed metastases of the prostate cancer extended with skip lesions along the corpus spongiosum in the entire anterior urethra (Fig. 1d). Moreover, he developed a catheter obstruction caused by hematuria, so a suprapubic cystostomy tube was placed and transurethral resection of the prostate (TURP) was performed to achieve tumor bleeding coagulation. Simultaneously, he underwent endoscopic resection of the urethra polyps. Histology showed metastasis of prostatic adenocarcinoma with aggressive variant (Fig. 1e, f, g, and h); particularly, as illustrated in Fig. 1e and f with immunolabeling for hematoxylin and eosin staining, the pathological findings of Case 1 exhibited a high-grade tumor defined by characteristic nuclear features, including lack of prominent nucleoli and high nuclear to cytoplasmic ratio. He was treated using cisplatin and etoposide. After two cycles, he achieved a progressive disease and he was treated with the best supportive care.
Fig. 1 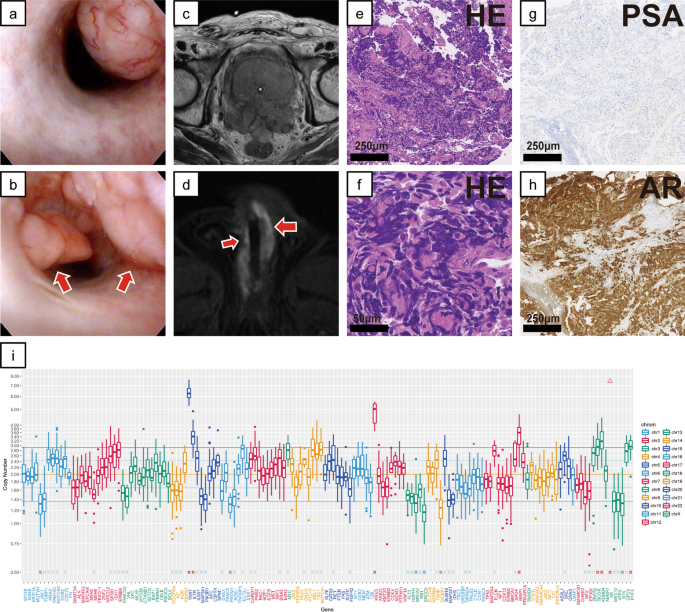
Cystoscopic, imaging, and pathological examination results and genomic sequencing in Case 1. a, b Cystoscopic findings in the urethra. The cystoscope shows several nodular polyps in the proximal penile urethra and distal bulbar urethra. c Prostate magnetic resonance imaging (MRI). The prostate was almost entirely replaced by the tumor, which has invaded the rectum. d MR image of the urethra. Metastases of the prostate cancer extended with skip lesions along the corpus spongiosum in the entire anterior urethra. e–h Representative microscopic images of hematoxylin and eosin (HE) staining and prostate-specific antigen and androgen receptor immunohistochemical staining of transurethral resections of urethra tumor specimens. These images were obtained using the following equipment: microscope, BX53; objective lens, UPLXAPO; camera, DP27; adapter, U-TV1XC. NanoZoomer-XR C12000 was used as acquisition software and the measured resolution was 500 dpi. i Examined genes (horizontal axis) and the copy number in Case 1 (vertical axis)
Targeted next-generation sequencing using an in-house assay of the resected specimen from the urethra polyps was performed (Additional file 1). A TP53 somatic point mutation (p.H193Y) was detected as a pathogenic variant. Gene amplification was detected in androgen receptor (AR) and KRAS (estimated copy number (CN): 35.3, 5.8, respectively). Loss of genetic heterozygosity (LOH) without mutation was observed in BRCA2. CN variation box (Fig. 1i) indicated a high LOH frequency, which is common in homologous recombination-deficient tumors.
-
Case 2. A 69 years old man was diagnosed with Gleason score 4 + 5 prostate cancer at another hospital. His serum PSA level was 81.5 ng/mL, and his clinical stage from CT and whole-body bone scans was T3aN1M1 (multiple lung and bone metastases). CAB therapy was started, and his PSA decreased to 0.36 ng/mL. However, after 1 year on androgen deprivation therapy (ADT), resistance to castration developed (PSA: 54.22 ng/mL), so docetaxel was started. For ten cycles of chemotherapy, his PSA decreased to a nadir of 17.2 ng/mL but subsequently increased to 84.0 ng/mL. MRI and CT of the abdomen and pelvis (Fig. 2a and b) showed non-muscle-invasive masses in the neck and urinary bladder posterior wall, although chest CT of the lung metastases showed partial responses (PRs). Cystoscopy showed bladder-neck obstruction by a tumor invading from the prostate gland (Fig. 2c) and revealed another group of nodular masses at the left posterior bladder wall (Fig. 2d). He was referred to our hospital for TURP and transurethral resection of the bladder tumor because of hematuria and urinary obstructive symptoms. Both pathological diagnoses of the bladder neck and posterior wall showed neuroendocrine differentiation prostate cancer (NEPC) (Fig. 2e, f, g, and h). Specifically, high mitotic rate cells were detected using immunolabeling for H&E staining, as illustrated in Fig. 2e, and the signals of synaptophysin were found in over 50% tumor cells (Fig. 2h). From the abovementioned points, we identified Case 2 as treatment-induced NEPC (tNEPC). He underwent two cycles of etoposide and carboplatin. However, the disease progressed, and the anticancer treatment was eventually discontinued.
Fig. 2 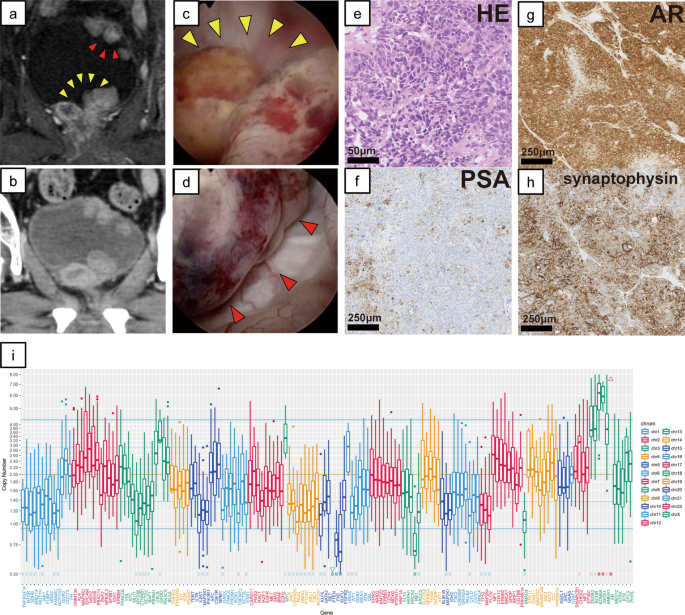
Cystoscopic, imaging, and pathological examination results and genomic sequencing in Case 2. a Bladder magnetic resonance imaging. b Pelvic computed tomography. Non-muscle-invasive masses in the neck and posterior wall of the urinary bladder are shown. c, d Cystoscopic findings. The tumor invaded from the prostate gland and has obstructed the bladder neck (c) and nodular masses are shown at the left posterior bladder wall (d). e–h Representative microscopic images of hematoxylin and eosin (HE) staining and prostate-specific antigen, androgen receptor, and synaptophysin immunohistochemical staining and transurethral resection of the bladder tumor specimens. These images were obtained using the following equipment: microscope, BX53; objective lens, UPLXAPO; camera, DP27; adapter, U-TV1XC. NanoZoomer-XR C12000 was used as acquisition software and the measured resolution was 500 dpi. i Examined genes (horizontal axis) and the copy number in Case 2 (vertical axis)


Targeted next-generation sequencing of the resected specimen from the posterior bladder posterior wall identified a TP53 somatic point mutation (p.R196P) as a pathogenic variant. Gene amplification was detected in AR (estimated CN: 25.4). Homozygous deletion was observed in PTEN, and LOH without mutation was observed in RB1. The CN variation box is shown in Fig. 2i.
Discussion and conclusion
Our two patients were initially diagnosed with prostate adenocarcinoma, which during hormonal treatment progressed with aggressive variant and neuroendocrine differentiation and multiple metastases to the urinary tract. NEPC occurs in 17% of patients with metastatic CRPC and has a poorer prognosis than other PCs [1, 3, 4]. NEPC tends to metastasize to bone, lung, and liver, and urethra or bladder metastasis has not been reported [1, 2]. Isolated metastasis or recurrence of PC in the intra-urinary tract is extremely rare, with only 15 cases reported previously [5,6,7,8,9,10,11,12,13,14,15,16,17,18,19] (Table 1); five had an origin in the prostatic ductal adenocarcinoma (PDC) and most of the rest were from adenocarcinomas with lower Gleason scores. On the other hand, in a study of 282 patients with secondary bladder neoplasms, 19% had PC-related secondary urinary bladder tumors [20], and 39% had urinary bladder metastases at autopsy [21], but the majority showed bladder-neck invasion. Case 2 may be the first report of adenocarcinoma with tNEPC as there are few case reports on isolated metastasis of PC to the bladder except for the bladder neck [22, 23].
From a genomic perspective, we wondered why these two cases progressed so quickly. Some patients with AIPC, including AVPC and tNEPC, respond to platinum-based combination chemotherapeutic regimens, but our patients were relatively treatment resistant. We actually performed targeted genomic sequencing of the formalin-fixed paraffin-embedded tumor specimens from TURP by applying algorithms previously reported [24, 25] and identified the factors common between the two patients: AR amplification and TP53 mutation (Figs. 1 and 2i). AR is overexpressed in most CRPC patients, and AR amplification means that these patients acquired castration resistance during cancer progression [26]. However, the fact was reported that in AIPC definition that the presence of AR amplification was irrelevant [2, 3]. In particular, our Case 1 patient showed KRAS amplification. Although KRAS mutation may be an advanced prostate cancer biomarker [27],the importance of KRAS amplification is uncertain. Progression of metastatic prostate cancer previously was coupled with enhanced expression levels of enhancer of zeste homolog, which is synergized by activation of KRAS and AR overexpression [28]. In Case 1, KRAS amplification may have been associated with accelerated de-differentiation to intractable NEPC. In Case 2, RB1 loss co-occurred with TP53 mutation. Previous studies have described that TP53 mutation cooperated with RB1 loss to confer an ADT-resistant phenotype, proposed as an aggressive variant prostate cancer [29, 30].
There are several hypotheses regarding the mechanisms of urethra metastasis, as in Case 1, including implantation following instrumentation or catheterization [11, 13]. Table 1 shows that previous patients with urethra metastasis had a history of post-TURP or prior radiotherapy for PC (or PDC), but our patient 1 did not respond. Additionally, because the tumor obstructed his urinary tract, he could not urinate smoothly with the self-catheter. Consequently, the mechanism for anterior urethra metastasis in Case 1 could have been direct surface implantation by self-catheterization. Regarding Case 2, it is probable that the mechanism of bladder metastasis was initial NEPC invasion of the bladder neck and subsequent posterior wall seeding. Metastasis from a urothelial carcinoma is well known, but the mechanism is unclear [31]. One hypothesis involves the seeding or intraepithelial spread of transformed cells [31, 32]. The spread from the primary tumor to the bladder wall in Case 2 may be similar to the spread of a urothelial carcinoma. These two cases also involved very interesting metastatic mechanisms.
Availability of data and materials
The data of targeted next-generation sequencing in two cases have been deposited to the Genome Sequence Archive (GSA). The assigned accession number is HRA002209. (https://bigd.big.ac.cn/gsa-human/browse/HRA002209).
Abbreviations
- PC:
-
Prostate cancer
- AIPC:
-
Androgen indifferent prostate cancer
- AVPC:
-
Aggressive variant prostate cancer
- NEPC:
-
Neuroendocrine differentiation prostate cancer
- PSA:
-
Prostate-specific antigen
- CAB:
-
Combined androgen blockade
- CRPC:
-
Castration-resistant prostate cancer
- c-TURP:
-
A channel transurethral resection of the prostate
- AR:
-
Androgen receptor
- LOH:
-
Loss of genetic heterozygosity
- ADT:
-
Androgen deprivation therapy
- PDC:
-
Prostatic ductal adenocarcinoma
References
Conteduca V, et al. Clinical features of neuroendocrine prostate cancer. Eur J Cancer. 2019;121:7–18.
Berchuck JE, Viscuse PV, Beltran H, Aparicio A. Clinical considerations for the management of androgen indifferent prostate cancer. Prostate Cancer Prostatic Dis. 2021;24:623–37.
Aggarwal R, et al. Clinical and genomic characterization of treatment-emergent small-cell neuroendocrine prostate cancer: a multi-institutional prospective study. J Clin Oncol. 2018;36:2492–503.
Epstein JI, et al. Proposed morphologic classification of prostate cancer with neuroendocrine differentiation. Am J Surg Pathol. 2014;38:756–67.
Haller B, Yao HH-I, Christidis D, Chee J, Bishop C. Clinical recurrence of prostatic ductal adenocarcinoma in the anterior urethra. J Clin Urol. 2020. https://doi.org/10.1177/2051415820921312.
Bryk DJ, Angermeier KW, Klein EA. A case of metastatic prostate cancer to the urethra that resolved after androgen deprivation therapy. Urology. 2019;129:e4–5.
Wang YG, Davies N, Desai D, Yap H-W. Local control of isolated anterior urethral metastasis from ductal prostate cancer. J Clin Urol. 2017;10:309–10.
Jhaveri H, Combs K, Jhaveri F. Direct extension of prostatic adenocarcinoma protruding through the urethral meatus. Urol Case Rep. 2017;13:13–5.
Zardawi I, Chong P. Metastatic prostate cancer to the urethra masquerading as urothelial carcinoma. Urol Case Rep. 2016;7:33–6.
Gómez Gómez E, Carrasco Aznar JC, Moreno Rodríguez Mdel M, Valero Rosa J, Requena Tapia MJ. Palliative surgery for rare cases of anterior urethral metastasis in prostate cancer. Case Rep Urol. 2014;2014:584957.
Beiko D, Zaza K, Power KV, Siemens DR, Boag AH. Isolated anterior urethral recurrence of prostatic adenocarcinoma. Can Urol Assoc J. 2014;8:E361-363.
Hung CF, et al. Invasive adenocarcinoma of the prostate with urethral tumor. J Chin Med Assoc. 2010;73:101–3.
Green JM, Tang WW, Jensen BW, Orihuela E. Isolated recurrence of ductal prostate cancer to anterior urethra. Urology. 2006;68(428):e413-425.
Nabi G, Devinder S, Dogra RN, Dinda AK. Malignant anterior urethral strictures: a rare complication of transurethral resection of malignant prostate. Int Urol Nephrol. 2002;34:73–4.
Ohyama C, et al. Adenocarcinoma arising from the prostatic duct mimicking transitional cell carcinoma. Int J Urol. 2001;8:408–11.
Kobayashi T, et al. Isolated recurrence of prostatic adenocarcinoma to the anterior urethra after radical prostatectomy. J Urol. 2000;164:780.
Taylor GB, McNeal JE, Cohen RJ. Intraductal carcinoma of the prostate metastatic to the penile urethra: a rare demonstration of two morphologic patterns of tumor growth. Pathology. 1998;30:218–21.
Aydin F. Endometrioid adenocarcinoma of prostatic urethra presenting with anterior urethral implantation. Urology. 1993;41:91–5.
Kotecha N, Gentile RL. Carcinoma of prostate with urethral metastasis. Urology. 1974;3:85–6.
Bates AW, Baithun SI. Secondary neoplasms of the bladder are histological mimics of nontransitional cell primary tumours: clinicopathological and histological features of 282 cases. Histopathology. 2000;36:32–40.
Saitoh H, et al. Metastatic patterns of prostatic cancer. Correlation between sites and number of organs involved. Cancer. 1984;54:3078–84.
Hallemeier CL, Kohli M, Chandan VS, Miller RC, Choo R. Multiple urinary bladder masses from metastatic prostate adenocarcinoma. Rare Tumors. 2010;2:e65.
Camilot D, Pizzolitto S, DeMaglio G, Falconieri G. Intravesical botryoid adenocarcinoma of the prostate: report of an unusual growth pattern of prostatic carcinoma simulating a urinary bladder tumor. Ann Diagn Pathol. 2007;11:413–6.
Mose LE, Wilkerson MD, Hayes DN, Perou CM, Parker JS. ABRA: improved coding indel detection via assembly-based realignment. Bioinformatics. 2014;30:2813–5.
Li H, Durbin R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics. 2009;25:1754–60.
Urbanucci A, et al. Overexpression of androgen receptor enhances the binding of the receptor to the chromatin in prostate cancer. Oncogene. 2012;31:2153–63.
Wang XS, et al. Characterization of KRAS rearrangements in metastatic prostate cancer. Cancer Discov. 2011;1:35–43.
Cai H, et al. Collaboration of Kras and androgen receptor signaling stimulates EZH2 expression and tumor-propagating cells in prostate cancer. Cancer Res. 2012;72:4672–81.
Ku SY, et al. Rb1 and Trp53 cooperate to suppress prostate cancer lineage plasticity, metastasis, and antiandrogen resistance. Science. 2017;355:78–83.
Nyquist MD, et al. Combined TP53 and RB1 loss promotes prostate cancer resistance to a spectrum of therapeutics and confers vulnerability to replication stress. Cell Rep. 2020;31:107669.
Habuchi T. Origin of multifocal carcinomas of the bladder and upper urinary tract: molecular analysis and clinical implications. Int J Urol. 2005;12:709–16.
Jones TD, et al. Molecular evidence supporting field effect in urothelial carcinogenesis. Clin Cancer Res. 2005;11:6512–9.
Acknowledgements
Yoko Suzuki, Emmy Yanagida, and Hiroshi Yamada provided technical assistance.
Funding
This study was supported in part by a Grant‐in‐Aid for Scientific Research (#20H03817 to T. Kosaka) from the Ministry of Education, Culture, Sports, Science and Technology of Japan. The study was supported in part by a research grant to T. Kosaka from the Fukuzawa Foundation of Keio University, Japan. The funding bodies played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the diagnosis and treatment of the patient. TM and TK prepared the manuscript and figures. HH, KY, and MO edited the manuscript, substantively revised it. KN and HN analyzed and interpreted the data of targeted next-generation sequencing. All authors have approved the submitted version and agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethical Committee of Keio University Hospital (#20160084 and #20180015). Written informed consent was obtained from the participants.
Consent for publication
Written consent has been obtained from both of the patients for publication of clinical details, radiological and biological data.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. How to perform the targeted next-generation sequencing using an in-house assay of the resected specimen.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Masuda, T., Kosaka, T., Nakamura, K. et al. Multiple metastases of androgen indifferent prostate cancer in the urinary tract: two case reports and a literature review. BMC Med Genomics 15, 118 (2022). https://doi.org/10.1186/s12920-022-01267-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12920-022-01267-z